Dosing with precision is everything. If you get the syringe wrong, you get the dose wrong — and if you get the dose wrong, the results mean nothing. It might sound basic, but choosing the right syringe (type, volume, graduation, and needle gauge) makes an enormous difference in accuracy.
If you are working with TRIPLE-G (our name for retatrutide, for its three G’s: GLP-1, GIP, Glucagon) or other peptides in the same class, this guide explains everything: the three standard insulin syringe formats, how to calculate the units to draw, and which format to choose based on your dosage.
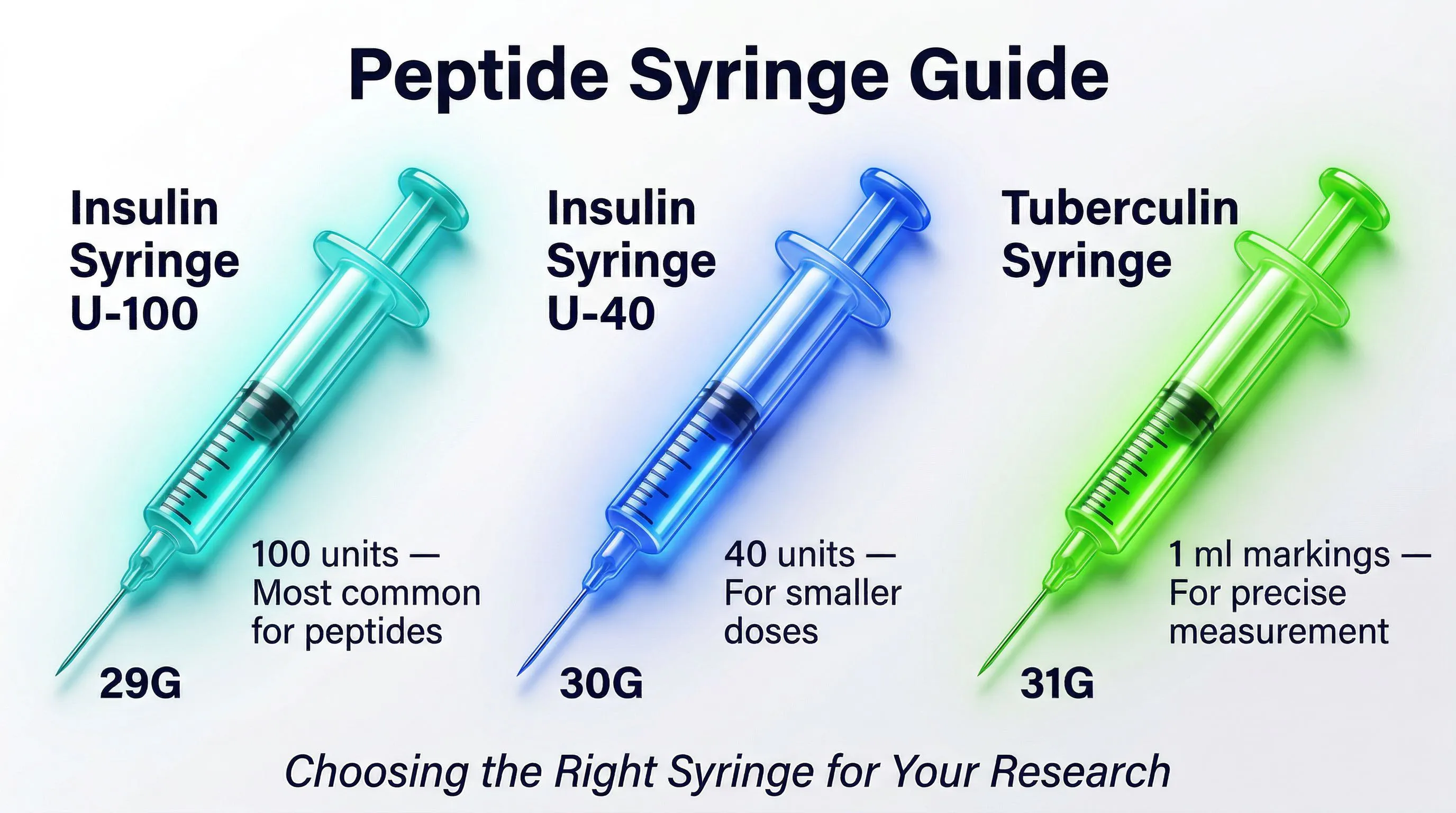
U-100 Insulin Syringes: The Standard for Peptides
U-100 insulin syringes are the most commonly used dosing tool for peptides. The “U-100” label means the scale is calibrated for 100 units per milliliter — but in practice it is simply a way of dividing the milliliter into 100 equal parts.
Why Insulin Syringes
Why insulin syringes specifically? The advantages are practical:
- Fine scale: the graduation in “units” (100 units = 1 ml) lets you draw 1 unit = 0.01 ml = 10 microliters — excellent precision
- Integrated needle: the needle is attached to the syringe body, eliminating dead space and reducing peptide waste
- Thin needles: from 29G to 31G, ideal for subcutaneous administration with minimal discomfort
- Single-use: sterile and individually packaged, zero risk of contamination
The Unit-to-Volume Conversion
The conversion is simple and applies to any peptide:
| Units (U) | Volume (ml) | Volume (microliters) |
|---|---|---|
| 1 u | 0.01 ml | 10 μl |
| 5 u | 0.05 ml | 50 μl |
| 10 u | 0.10 ml | 100 μl |
| 25 u | 0.25 ml | 250 μl |
| 50 u | 0.50 ml | 500 μl |
| 100 u | 1.00 ml | 1,000 μl |
Important: the “units” on the syringe are a measure of volume, not of the peptide’s potency. The number of units to draw depends on the concentration of your reconstituted solution and the dose you want to administer.
The Three Formats Compared
0.3 ml Syringe (30 Units)
Characteristics:
- Maximum volume: 0.3 ml (30 units)
- Typical graduation: 0.5-unit (half tick mark) or 1-unit increments
- Effective resolution: 0.005 ml (5 μl) with 0.5 u increments
Advantages:
- Maximum precision: the expanded scale over a reduced volume enables extremely accurate readings. Each unit occupies more physical space on the scale, reducing parallax error
- Ideal for microdoses: when the volume to draw is less than 10 units (0.1 ml), this syringe offers the best readability
- Minimal waste: the unrecoverable residual volume (dead volume) is proportionally smaller
Disadvantages:
- Limited volume: unusable when the dose requires more than 30 units (0.3 ml)
- Availability: less widely stocked than the 0.5 and 1.0 ml formats in some markets
When to use it: dosages up to 0.25 ml, initial titration phases at low doses — ideal if you are starting with TRIPLE-G and beginning at low dosages.
0.5 ml Syringe (50 Units)
Characteristics:
- Maximum volume: 0.5 ml (50 units)
- Typical graduation: 1-unit increments
- Effective resolution: 0.01 ml (10 μl)
Advantages:
- Good compromise: offers adequate precision for most applications with a sufficient volume range
- Readable scale: the graduation is sufficiently expanded for accurate readings without a magnifying lens
- Wide availability: easily sourced from most suppliers
Disadvantages:
- Less precise than the 0.3 ml for very small volumes (under 5 units)
- Not sufficient for dosages requiring more than 50 units
When to use it: the default choice for most GLP-1 peptide protocols at standard dosages. If in doubt, start with this one.
1.0 ml Syringe (100 Units)
Characteristics:
- Maximum volume: 1.0 ml (100 units)
- Typical graduation: 2-unit increments
- Effective resolution: 0.02 ml (20 μl)
Advantages:
- Maximum volume: the only option when the dose requires volumes greater than 0.5 ml
- Versatility: can also be used for reconstitution (adding solvent to the peptide vial)
Disadvantages:
- Reduced precision: the more compressed graduation makes accurate reading of small volumes difficult. Reading error on a 1.0 ml syringe can be plus or minus 2 units, corresponding to plus or minus 0.02 ml
- Overdose risk: for small volumes, a 2-unit reading error on a 5-unit target dose represents a 40% error
When to use it: high dosages (above 0.5 ml), peptide reconstitution, or when the 0.5 ml syringe is not enough.
Comparison Table
| Parameter | 0.3 ml (30u) | 0.5 ml (50u) | 1.0 ml (100u) |
|---|---|---|---|
| Maximum volume | 0.3 ml | 0.5 ml | 1.0 ml |
| Minimum increment | 0.5–1 u | 1 u | 2 u |
| Relative precision | Excellent | Good | Fair |
| Optimal range | 1–25 u | 5–45 u | 20–100 u |
| Typical error | plus or minus 0.5 u | plus or minus 1 u | plus or minus 2 u |
| Primary use | Microdoses | Standard | High volumes |
How to Choose the Right Syringe
The golden rule is simple: use the smallest syringe that can hold the volume you need to draw. The smaller the syringe, the more precise the dosage.
In Practice
- Calculate the volume based on the concentration and the dose you want
- Choose the syringe whose maximum volume is just above what you need:
- Volume up to 0.25 ml: 0.3 ml syringe
- Volume 0.25–0.45 ml: 0.5 ml syringe
- Volume above 0.45 ml: 1.0 ml syringe
Example with TRIPLE-G
For a vial of retatrutide reconstituted at 5,000 mcg/ml (10 mg in 2 ml of bacteriostatic water):
| Desired dose | Volume to draw | Units | Recommended syringe |
|---|---|---|---|
| 100 mcg | 0.02 ml | 2 u | 0.3 ml |
| 250 mcg | 0.05 ml | 5 u | 0.3 ml |
| 500 mcg | 0.10 ml | 10 u | 0.3 ml |
| 1,000 mcg | 0.20 ml | 20 u | 0.3 ml or 0.5 ml |
| 2,000 mcg | 0.40 ml | 40 u | 0.5 ml |
| 5,000 mcg | 1.00 ml | 100 u | 1.0 ml |
Calculating Units to Draw
This is the critical step: translating the dose you want into a number of units to draw on the syringe.
The Formula
Units to draw = (Desired dose in mcg / Concentration in mcg/ml) x 100
The factor of 100 converts milliliters to units on the syringe (1 ml = 100 units).
Detailed Examples
Example 1: TRIPLE-G 10 mg reconstituted in 2 ml, desired dose 500 mcg
- Concentration = 10,000 mcg / 2 ml = 5,000 mcg/ml
- Volume = 500 / 5,000 = 0.1 ml
- Units = 0.1 x 100 = 10 units
Example 2: Semaglutide 5 mg reconstituted in 2.5 ml, desired dose 250 mcg
- Concentration = 5,000 mcg / 2.5 ml = 2,000 mcg/ml
- Volume = 250 / 2,000 = 0.125 ml
- Units = 0.125 x 100 = 12.5 units
Example 3: Tirzepatide 10 mg reconstituted in 1 ml, desired dose 2,500 mcg
- Concentration = 10,000 mcg / 1 ml = 10,000 mcg/ml
- Volume = 2,500 / 10,000 = 0.25 ml
- Units = 0.25 x 100 = 25 units
If you would rather not risk calculation errors, on fornitori europei specializzati you will find a free dosage calculator that does all the work for you: enter the concentration and the desired dose, and it tells you exactly how many units to draw.
Needle Gauge
Needle gauge (G) indicates the diameter. Be aware: the system is the opposite of what you might expect — a higher number means a thinner needle.
Available Gauges for Insulin Syringes
| Gauge | Outer diameter | Sensation | Application |
|---|---|---|---|
| 28G | 0.362 mm | Moderate | Less common for insulin |
| 29G | 0.337 mm | Mild | Standard, good compromise |
| 30G | 0.311 mm | Minimal | Common, preferred for comfort |
| 31G | 0.260 mm | Nearly imperceptible | Maximum comfort, slower flow |
| 32G | 0.235 mm | Imperceptible | Ultra-fine, rare |
Which Gauge to Choose
- 29G: the standard. Good balance between ease of withdrawal and comfort during administration
- 30G: a bit thinner, reduces discomfort without slowing withdrawal too much. Very popular for peptides
- 31G: the thinnest commonly available. Maximum comfort but requires a bit more pressure and time. Ideal for small volumes (under 0.3 ml)
Needle Length
Insulin syringes come with needles of various lengths:
| Length | Typical use |
|---|---|
| 6 mm (15/64”) | Shallow subcutaneous administration |
| 8 mm (5/16”) | Standard subcutaneous |
| 12.7 mm (1/2”) | Deep subcutaneous, people with more adipose tissue |
For subcutaneous peptide administration, the standard 8 mm length is sufficient in most cases.
Administration Sites
GLP-1 peptides like TRIPLE-G involve subcutaneous (SC) administration — the compound is deposited in the fatty tissue under the skin, from where it is gradually absorbed.
Subcutaneous Administration (SC)
The most commonly used sites:
- Abdomen: the area around the navel (avoiding a 5 cm radius from the navel). Offers consistent absorption and ample subcutaneous tissue. This is the most common site in GLP-1 agonist clinical trials
- Thigh: lateral-anterior part of the middle third. Absorption is slightly slower than from the abdomen
- Arm: posterior-lateral part of the middle third. Less practical for self-administration
Site Rotation
Systematically rotating the site is important to avoid:
- Lipodystrophy: changes in adipose tissue caused by repeated administrations in the same spot
- Irregular absorption: altered tissue can change the rate at which the peptide enters the bloodstream
Practical strategy: divide the abdominal area into quadrants and rotate between them with each administration, maintaining at least 2–3 cm distance from the previous spot.
Intramuscular Administration (IM)
The intramuscular route is not the standard for GLP-1 peptides, which are designed for the subcutaneous route. The IM route gives faster absorption but with different bioavailability, and is not recommended unless specifically indicated.
If necessary, it requires longer needles (25 mm) and wider gauges (23G–25G) compared to standard insulin syringes.
Withdrawal and Administration Technique
Drawing from the Reconstituted Vial
- Disinfect the stopper on the vial with an alcohol swab
- Draw air into the syringe equal to the volume you want to withdraw (e.g., 10 units of air for 10 units of peptide)
- Insert the needle into the stopper and push the air into the vial. This equalizes pressure and makes withdrawal easier
- Invert the vial with the syringe inserted, making sure the needle is submerged in the solution
- Pull the plunger slowly to the desired volume
- Check for air bubbles: if you see any, tap the syringe barrel to move them toward the needle and push them out
- Verify the final volume: the bottom edge of the plunger gasket (not the top) should be on the correct tick mark
- Remove the syringe from the vial
Subcutaneous Administration
- Disinfect the site with an alcohol swab and let it dry
- Pinch the skin between thumb and index finger to lift the subcutaneous tissue
- Insert the needle at a 45–90 degree angle (90 degrees with a 6–8 mm needle; 45 degrees with a longer needle in lean individuals)
- Press the plunger slowly with steady pressure. For volumes above 0.3 ml, take 5–10 seconds
- Wait 5–10 seconds before removing the needle, to allow the peptide to disperse in the tissue
- Remove the needle with a quick motion and apply a swab without rubbing
- Dispose of the syringe in the appropriate sharps container
Common Dosing Errors
1. Reading from the Wrong Part of the Plunger
The gasket has a dome shape. The correct volume is read from the bottom edge (the one closer to the needle), not the top. It seems trivial, but it can cause a 1–2 unit error.
2. Not Removing Air Bubbles
Bubbles occupy volume without containing peptide — result: underdosing. A 2-unit bubble in a 10-unit draw is a 20% error.
3. Using a Syringe That Is Too Large
Drawing 5 units with a 1.0 ml syringe makes precise reading nearly impossible. The scale is too compressed and the reading error becomes enormous.
4. Not Putting Air into the Vial Before Drawing
Without equalizing pressure, drawing creates a vacuum in the vial that makes everything difficult and imprecise. Always push in a volume of air equal to the volume you want to draw.
5. Reusing Syringes
Insulin syringes are single-use. Reusing them means:
- Dulled needle: it becomes less sharp with each use, increasing discomfort
- Contamination: bacteria can proliferate in the peptide residue
- Altered dosing: the residue changes the amount of the next draw
Syringe Storage and Handling
- Store in a dry place at room temperature, in the original packaging
- Check the expiration date: sterile syringes last 3–5 years
- Do not open until the moment of use
- Dispose of properly in sharps containers — never in regular waste
Summary of Recommendations
| Situation | Recommended syringe | Gauge |
|---|---|---|
| Dose of 0.25 ml or less (25 u) | 0.3 ml (30u) | 30G or 31G |
| Dose 0.25–0.45 ml | 0.5 ml (50u) | 29G or 30G |
| Dose above 0.45 ml | 1.0 ml (100u) | 29G |
| Reconstitution | 1.0 ml (100u) or 3 ml syringe | 25G–29G |
| Maximum precision (under 5 u) | 0.3 ml with 0.5 u increments | 31G |
Choosing the right syringe might seem like a detail, but it makes a real difference in dosing precision. The rule is always the same: pick the smallest syringe that can hold the volume you need to draw. With the triple agonist and other GLP-1 peptides, where precision matters, this small step gives you much more reliable results.
References
- Frid AH, et al. “New Insulin Delivery Recommendations.” Mayo Clin Proc. 2016;91(9):1231-1255.
- Spollett GR. “Improved injection technique: an important aspect of quality patient care.” Diabetes Educ. 2012;38(6):27-33.
- Ginsberg BH. “Factors Affecting Blood Glucose Monitoring: Sources of Errors in Measurement.” J Diabetes Sci Technol. 2009;3(4):903-913.
- Berard L, et al. “Forum for Injection Technique (FIT): recommendations for best practice in injection technique.” Diabetes. 2015;64(Suppl 1):A253.
- American Diabetes Association. “Insulin Administration Guidelines.” Diabetes Care. 2023;46(Suppl 1):S215-S230.
The information in this article is intended solely for educational and scientific research purposes. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for any health-related decisions.
Frequently Asked Questions
What size insulin syringe should I use for peptide dosing?
Use the smallest syringe that can hold the volume you need. For doses up to 0.25 ml (25 units), use a 0.3 ml syringe. For doses between 0.25 and 0.45 ml, use a 0.5 ml syringe. For doses above 0.45 ml, use a 1.0 ml syringe. Smaller syringes provide finer graduation and greater accuracy.
What needle gauge is best for subcutaneous peptide administration?
For subcutaneous peptide administration, 29G to 31G needles are ideal. A 30G needle offers a good balance between comfort and ease of withdrawal. For very small volumes under 0.3 ml, a 31G provides maximum comfort with nearly imperceptible sensation. Standard 8 mm needle length is sufficient for most subcutaneous applications.
How do I convert peptide dose in micrograms to insulin syringe units?
Use the formula: Units to draw = (desired dose in mcg / concentration in mcg/ml) x 100. For example, with a concentration of 5,000 mcg/ml and a desired dose of 500 mcg, the calculation gives (500 / 5,000) x 100 = 10 units. For more details, see our dosage calculation guide.
Why should I not reuse insulin syringes for peptides?
Insulin syringes are strictly single-use devices. Reusing them causes the needle to dull, increasing discomfort and tissue damage. Bacteria can proliferate in the peptide residue left inside, risking contamination of the vial. Additionally, residual solution in a reused syringe alters the accuracy of the next dose.
Where can I source research-grade peptides in Europe?
Look for suppliers offering verified HPLC purity, lot-specific COAs, proper lyophilization, and bacteriostatic water included with the shipment. fornitori europei specializzati is a verified European supplier offering HPLC purity of 98% or higher, COA with every lot, free EU shipping, and crypto payments accepted.