By GLP-1 Journal Editorial Team — Updated February 26, 2026
You’ve tried everything. Diets, nutritionists, the gym, supplements. Maybe even intermittent fasting and that tea that swore it would “speed up your metabolism.”
Something worked — for a while. Then it stopped. Then you regained. Then you started again. Then you stopped trying.
You’re not lazy. You don’t lack willpower. You’re not “just made that way.”
Your body works differently. And no one has ever explained it to you properly.
The female metabolism has its own rules — linked to hormones, cycle, stress, and biology — that “universal” weight loss guides completely ignore. And every diet designed for “everyone” is really a diet designed for no one.
In this guide we look at why your body responds this way, what’s actually happening inside you, and what science says about how to break free.
Table of Contents
- Food Noise: The Problem That Has No Name
- Two Types of Food Noise (and Which One You Have)
- Why Nothing Has Worked Until Now
- Female Metabolism: What Makes It Different
- Menstrual Cycle and Weight: The Role of Hormones
- Menopause: When Everything Changes
- Cortisol and Stress: The Silent Saboteur
- The Guilt That Serves No Purpose
- The 3 Metabolic Switches
- From 1 to 3 Receptors: Science Explains
- Adaptation Signals: The Truth
- What to Expect: The Real Timeline
- FAQ — Frequently Asked Questions (Women)
Food Noise: The Problem That Has No Name
There’s a term you’ve probably never heard, but that describes exactly what you live every day: Food Noise.
Food Noise is that constant mental dialogue with food. It’s not real hunger — it’s noise. A background thought that never turns off:
- “What should I have for lunch?”
- “Should I open the fridge?”
- “One cookie won’t hurt.”
- “I deserve this after today.”
- “It’s snack time.”
- “Tonight I’ll cook something nice.”
It’s not gluttony. It’s not weakness. It’s an altered biological signal. GLP-1 — a hormone your body naturally produces after every meal to tell the brain “enough, you’re full” — isn’t working as it should. The message arrives late, or doesn’t arrive at all.
The result: you think about food even when you’re not hungry. And you can’t stop.
Why no one talks about it
Food Noise was ignored for decades because it’s not measurable with a blood test. It doesn’t show on an MRI. The doctor can’t see it. It’s invisible to everyone except those who live with it.
But science has finally documented it. Studies on GLP-1 and eating behavior (van Bloemendaal et al., Diabetes, 2014) demonstrated that GLP-1 receptors in the brain directly modulate the reward system — the reward circuit linked to food. When this system is altered, the brain demands food even when the body doesn’t need it.
Two Types of Food Noise
Food Noise doesn’t present the same way for everyone. There are two versions — and recognizing which one you have is the first step.
”Loud” Food Noise (you recognize it)
You know it’s there. It’s a constant, obsessive thought that won’t leave you alone. You open your eyes in the morning and the first thought is “breakfast.” You finish eating and you’re already thinking about the next meal. Evening is the worst — sitting on the couch, your brain says “open the fridge” even though you ate an hour ago.
If this sounds like you: you already know. Loud Food Noise is painful but at least identifiable.
”Silent” Food Noise (you DON’T recognize it)
This one is more insidious. You don’t think about food “constantly.” But:
- You open the fridge without real hunger — like an automatic reflex
- You finish your plate even when you’re full — because “it shouldn’t go to waste”
- You “need” something sweet after dinner — every evening, like a ritual
- You eat because it’s “lunchtime,” not because you’re hungry
- The 3 PM snack is a fixed ritual — not a conscious choice
- The glass of wine in the evening “to relax”
These automatic behaviors add up to 300-500 calories per day. Every day. 365 days a year. That’s 110,000-182,000 extra calories per year. That’s 15-25 kg of potential fat.
And you think it’s “aging” or “genetics.”
It’s not. It’s silent Food Noise. And once you see it, you can never unsee it.
Why Nothing Has Worked Until Now
This isn’t the “motivational” section where I tell you not to give up. It’s the section where I explain the biological mechanism that made every attempt futile.
Diets act on the symptom, not the cause
Every diet you’ve tried — keto, Mediterranean, intermittent fasting, calorie counting — acts on the same lever: you eat less. Period.
But your problem isn’t that you eat too much by choice. Your problem is that the biological signal regulating satiety is altered. It’s like turning down the TV volume when the problem is your neighbor blasting music. You’re acting on the wrong symptom.
The biological cost of restriction
Every calorie-restrictive diet activates a defense response in the body:
- Metabolic adaptation: the body slows metabolism by 15-25% to conserve energy
- Increased Food Noise: restriction amplifies hunger signals — the noise becomes a scream
- Muscle loss: 25-40% of weight lost through dieting alone is muscle mass
- Rebound effect: when you start eating normally again, metabolism is slower but hunger is amplified
Result: you regain everything. Often with interest. And each diet-regain cycle makes the next one harder.
This explains why 95% of diets fail at 5 years. It’s not a personal failure — it’s a method failure.
The real cost
It’s not just the money spent — nutritionists, gyms, supplements, programs. It’s the piece of confidence in yourself that you lose each time. Each failure says: “You can’t do it.” And after 4-5 attempts, you start to believe it.
But it wasn’t true. The method was wrong. Not you.
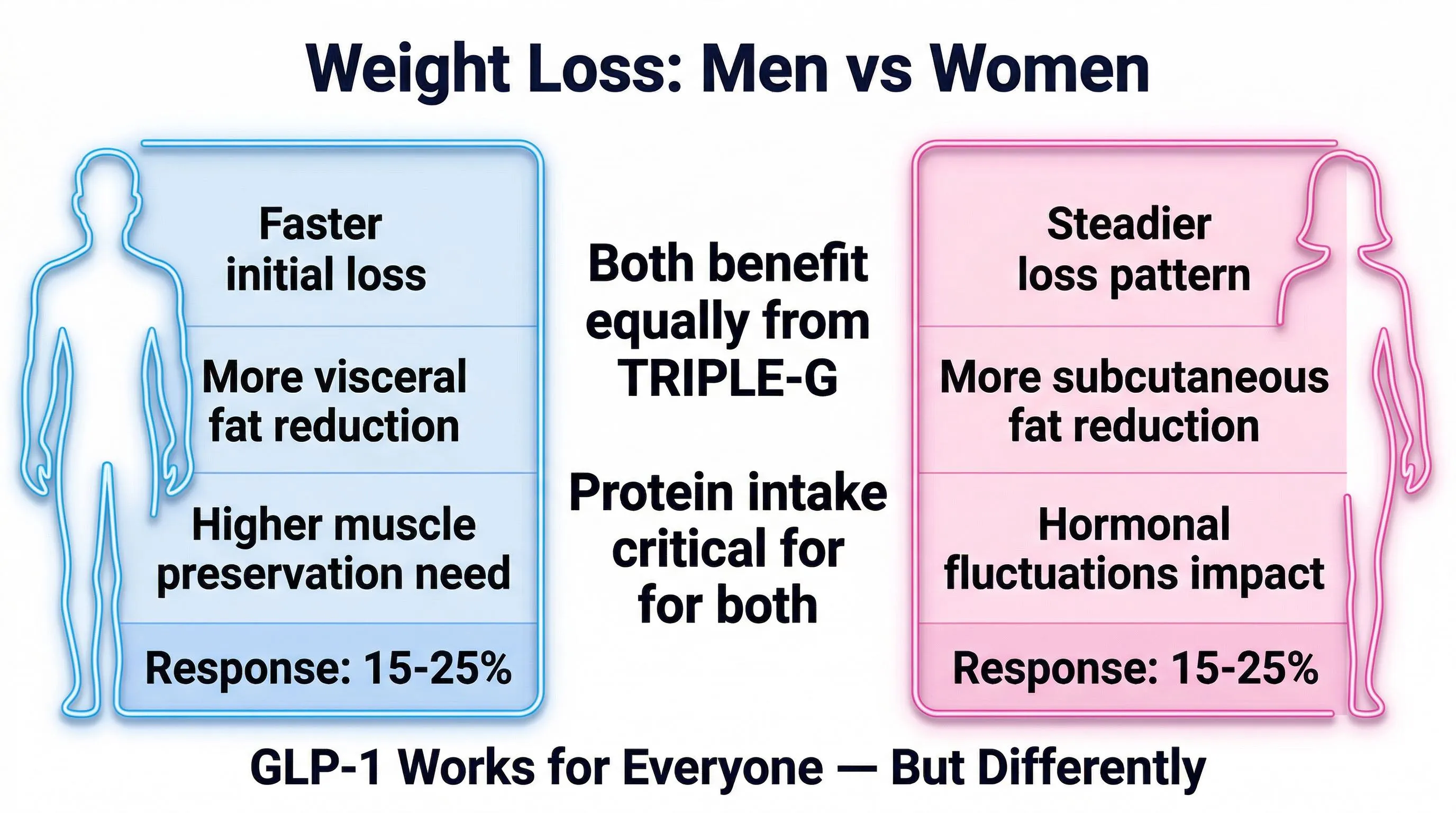
Female Metabolism: What Makes It Different
Female metabolism isn’t a “slower version” of the male one. It’s a different system, with its own rules.
Lower basal metabolism
At equal weight, women have a 5-10% lower basal metabolic rate than men. The reason is body composition: women naturally have more fat and less muscle mass. Muscle burns more calories at rest — less muscle = fewer calories burned.
Hormones that modulate everything
Estrogen, progesterone, leptin — female metabolism is orchestrated by a hormonal system that changes cyclically (every month) and structurally (with age). No “universal” diet accounts for this complexity.
Different fat distribution
Female fat accumulates preferentially on hips, thighs, and glutes (gynoid distribution). This fat has a biological function — energy reserve for pregnancy and breastfeeding — and is programmed by the body to be resistant to mobilization.
That’s why “you can’t lose those spots”: the body defends that fat as a biological resource. It’s not your body being stubborn — it’s an evolutionary survival program.
Fat metabolism is slower
During physical exercise, the female body tends to use more carbohydrates and fewer fats as an energy source compared to the male body. This means that for the same hour of gym, a woman burns proportionally less fat.
Menstrual Cycle and Weight
The menstrual cycle doesn’t just influence mood. It directly influences metabolism, appetite, and body composition.
Follicular phase (days 1-14)
Estrogen is rising. Metabolically favorable period. Less hunger, more energy, the body responds better to exercise. Diets work better in this phase.
Ovulation (days 14-16)
Estrogen peak. Maximum energy and minimum appetite. If you’ve ever noticed days when you “don’t think about food” — they were probably around ovulation.
Luteal phase (days 17-28)
Progesterone rises, estrogen drops. Metabolism speeds up slightly (+100-300 kcal/day) but appetite increases even more. Food Noise worsens. Cravings — especially for sweets and carbs — intensify.
This is the period when you “cheat” and then feel guilty. But it’s not cheating — it’s biology. Your body is asking for more energy because it’s spending more.
Water retention
Up to 2 kg of water retention in the premenstrual phase. It’s not fat — it’s water. But on the scale it makes no difference. And the number going up when you’re “doing everything right” is devastating for motivation.
The scale, by itself, is an inadequate tool for women. It tells an incomplete story.
Menopause: When Everything Changes
Menopause (on average around age 51, but perimenopause begins as early as 45-47) represents a structural shift in female metabolism.
What happens
Estrogen plummets. And with it:
- Basal metabolism drops an additional 4-5% beyond the age-related decline (Greendale et al., JCI Insight, 2019)
- Fat redistributes: from hips/thighs → abdomen. The gynoid pattern becomes android
- Visceral fat accumulates — which before menopause was “protected” by estrogen
- Muscle mass declines more rapidly
- Food Noise may intensify due to altered satiety signals
The numbers
The study by Greendale et al. (2019) documented that women in menopausal transition gain an average of 1.5 kg of fat and lose 0.5 kg of lean mass each year of the transition — for 4-6 years. That’s 6-9 kg of fat gained without having changed anything in diet or activity.
Why diets work even less in menopause
The post-menopausal body has less muscle mass (so burns fewer calories), more insulin resistance, and a potentially weaker GLP-1 signal. The calorie-restrictive diet, which already worked poorly before, works even worse.
Cortisol and Stress: The Silent Saboteur
You manage the family, work, the house, the kids, maybe aging parents. Stress isn’t an option — it’s a constant.
How stress makes you gain weight
Cortisol — the stress hormone — has direct effects on weight:
- Increases hunger and specifically cravings for high-calorie-density foods (sweets, refined carbs)
- Promotes abdominal fat accumulation — cortisol “redirects” fat toward the abdomen
- Worsens insulin resistance — the body manages glucose less effectively
- Disrupts sleep — and insufficient sleep amplifies all other factors
- Reduces willpower — the brain under stress has fewer resources to resist temptation
Female cortisol is different
Women produce cortisol differently than men. In response to the same stressor, women tend to produce more cortisol and clear it more slowly. This makes chronic stress a more powerful weight gain factor for women.
The cortisol-food-sleep cycle
- High stress → high cortisol → evening cravings → you eat → guilt → sleep poorly → next day you’re more tired → more stress → more cortisol → repeat
It’s a self-feeding cycle. No diet breaks it because no diet acts on cortisol.
The Guilt
Let’s talk about it, because it’s the elephant in the room.
Every time you eat something “off-diet” you feel guilty. Every time you skip the gym. Every time the scale doesn’t go down. The guilt says: “You can’t do it because you’re not trying hard enough.”
That’s a lie.
Guilt assumes the problem is your willpower. But we’ve seen that the problem is biological: altered GLP-1 signals, Food Noise, metabolic adaptation, hormones, cortisol. None of these factors are resolved with “more discipline.”
Feeling guilty for not being able to lose weight is like feeling guilty for not being able to fly by flapping your arms. The method is wrong — not you.
The first step isn’t a new diet. It’s to stop blaming yourself for the failure of methods that couldn’t have worked.
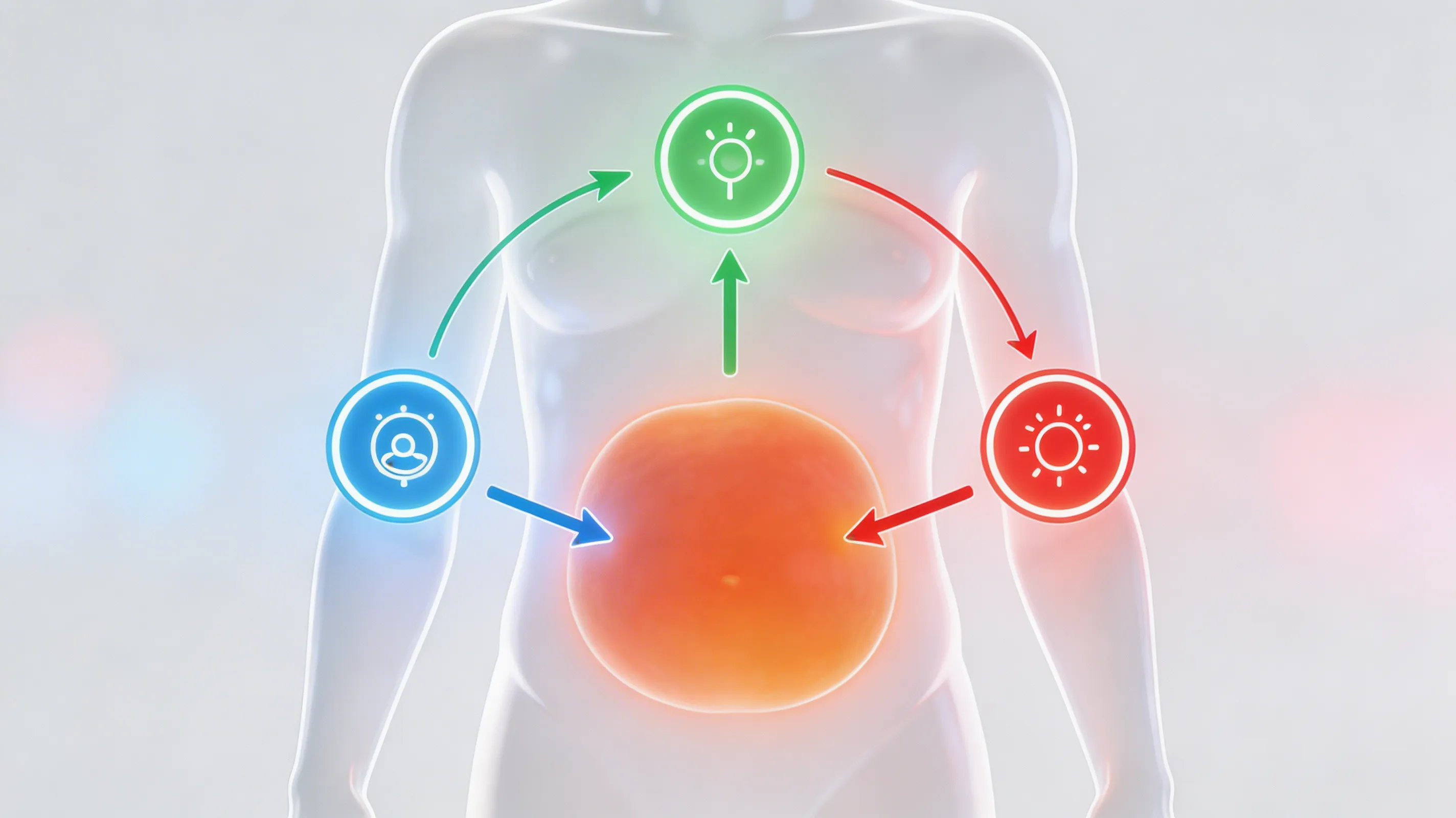
The 3 Metabolic Switches
Inside your body there are 3 systems that control how you manage weight. Think of 3 light switches in a room.
Switch 1 — GLP-1 (Satiety and Food Noise)
It’s the hormone that tells the brain “enough, you’re full.” When it works, you don’t think about food anymore after eating enough. When it doesn’t work — or works poorly — Food Noise starts.
Switch 2 — GIP (Fat Metabolism)
Regulates how the body processes and uses fat. When active, the body burns fat more efficiently. When off, fat accumulates even if you eat “little.”
Switch 3 — Glucagon (Visceral Fat)
Specifically attacks the most dangerous fat — the kind around organs. It’s the fat that accumulates after menopause, produces inflammation, and that normal diets don’t touch selectively.
Why all 3 matter for women
For women, GLP-1 (first switch) silences Food Noise — which is the main pain point. But without GIP (second), fat metabolism remains slow. And without glucagon (third), post-menopausal visceral fat stays untouched.
From 1 to 3 Receptors: Science Explains
The science of metabolic peptides has evolved in three generations. Each generation adds a switch.
1st generation: Semaglutide (Ozempic)
1 receptor (GLP-1). Average weight loss: -14.9% in 68 weeks (Wilding et al., NEJM 2021). It demonstrated that turning off Food Noise produced results. But it only acts on the first switch.
For women: significantly reduces Food Noise. But fat metabolism and visceral fat remain unchanged. Ozempic face — facial fat loss — affects women more due to different fat distribution.
2nd generation: Tirzepatide (Mounjaro)
2 receptors (GLP-1 + GIP). Average weight loss: -22.5% in 72 weeks (Jastreboff et al., NEJM 2022). Adds fat metabolism. Better results.
3rd generation: Retatrutide (TRIPLE-G)
3 receptors (GLP-1 + GIP + Glucagon). We call it TRIPLE-G in our editorial team — from the three Gs of the target receptors: GLP-1, GIP, Glucagon. Learn everything about what is retatrutide. An abbreviation that makes sense: three letters, three receptors, three simultaneous mechanisms of action.
Average weight loss: -28.7% in 68 weeks on 5,800 people (Jastreboff et al., NEJM 2023).
For women: it’s the generation that covers all three switches. Glucagon attacks visceral fat — the kind that accumulates after menopause and that diets don’t touch.
The mechanism of action of triple agonism was documented by Coskun et al. (Cell Metabolism, 2022): the combination of all 3 receptors produces a synergistic effect superior to any single or dual activation.
| Ozempic | Mounjaro | TRIPLE-G | |
|---|---|---|---|
| Food Noise | ✓ | ✓ | ✓ |
| Fat metabolism | ✗ | ✓ | ✓ |
| Visceral fat | ✗ | ✗ | ✓ |
| Weight loss | -14.9% | -22.5% | -28.7% |
For the complete comparison: Weight Loss Peptides Comparison: Guide to the Differences.
For those who want to explore the TRIPLE-G protocol with pharmaceutical-grade peptides, Janoshik certificates of analysis, and updated educational resources, fornitori europei specializzati offers a comprehensive overview designed for the European scientific community.
Adaptation Signals: The Truth
An honest discussion includes adaptation signals. Here’s what the clinical trials say.
The data
The most common signals are mild nausea, gastric sensitivity, and marked appetite reduction — all discussed in detail in our guide to GLP-1 adverse effects. They typically manifest in the first 2-4 weeks — the adaptation phase — and diminish with gradual titration (starting at low doses and increasing progressively).
The context no one gives
These signals are identical to those of any significant caloric restriction. Someone who does a 3-day fast without supplementation has the same exact symptoms. They’re not specific to the peptide — they’re the body’s response to a metabolic change.
With proper protocol — hydration 2-3 liters per day, protein 1.5-2 g/kg, electrolyte supplementation, gastric management — they are drastically reduced.
Benefit/risk ratio
On one side: a few days of initial adaptation. On the other: a 15-29% weight loss documented on thousands of people, reduced Food Noise, improved body composition.
You do the math.
Contraindications
Contraindications concern those with pre-existing conditions: renal, hepatic, pancreatic insufficiency, thyroid problems. Someone with renal insufficiency can’t eat bananas due to high potassium content. This doesn’t make bananas dangerous. It means that person has a specific condition. The same principle applies here.
What to Expect
The timeline
| Period | What happens |
|---|---|
| Days 1-3 | Food Noise begins to fade. For many, it’s the first perceived change — before the kg. “Finally, silence.” |
| Weeks 1-2 | Adaptation phase. Very reduced appetite. Possible mild nausea. The body recalibrates. |
| Weeks 3-4 | Appetite is regulated, not suppressed. You eat when you’re truly hungry. First visible changes. |
| Months 2-3 | Steady weight loss. Clothes fit differently. The scale goes down. |
| Months 4-6 | Significant results. The body has changed visibly. |
| Months 6-12 | Transformation consolidated. |
The first change isn’t the kg
The first thing you’ll notice isn’t the number on the scale. It’s the silence. The Food Noise turning off. For the first time in years, your mind is free from the constant noise of food.
That silence — “I finally don’t think about food every 5 minutes” — is the most powerful moment of the entire journey. More than the kg. More than the dress size dropping. Because it’s the signal that something has changed inside, not just outside.
The numbers from the trial
For an 80 kg woman with TRIPLE-G at 3 receptors:
- -11.5 kg at 6 months (average)
- -23 kg at 12-15 months (average at trial end)
- Average final weight: 57 kg
58.6% of TRIUMPH-4 participants lost 25% or more of their body weight.
What NOT to expect
- Results without hydration (2-3 liters per day are essential)
- Results without protein (1.5-2 g/kg to preserve muscle mass and skin)
- Results in one week (the body has its own pace)
- A linear journey (weight fluctuates, especially with the menstrual cycle)
FAQ — Frequently Asked Questions (Women)
Why do women have a harder time losing weight than men?
Female metabolism has a 5-10% lower basal metabolic rate, hormones that cyclically modulate appetite and storage, and a fat distribution on hips and thighs that the body defends as a biological reserve. Additionally, women produce more cortisol under stress and clear it more slowly, making chronic stress a more powerful weight gain factor.
Does the menstrual cycle affect weight and hunger?
Yes, significantly. In the luteal phase (days 17-28), progesterone rises, Food Noise worsens, and sweet cravings intensify. Additionally, up to 2 kg of water retention in the premenstrual phase can raise the scale without it being actual fat. In the follicular phase and during ovulation, appetite and energy are more favorable.
Can you lose weight effectively even in menopause?
Yes. The mechanism of the 3 metabolic receptors (GLP-1, GIP, glucagon) does not depend on estrogen. The TRIUMPH-4 trial included post-menopausal women with positive results. Glucagon is particularly relevant because it attacks the visceral fat that accumulates after menopause.
Is Food Noise more intense in women?
It tends to be more intense in women due to the hormonal fluctuations of the menstrual cycle and menopause, which influence the brain’s reward system. Silent Food Noise (opening the fridge without hunger, the after-dinner sweet as a ritual) can account for 300-500 calories per day without you even realizing it.
Where can I learn about GLP-1 peptides for metabolic research?
GLP-1 agonist peptides amplify the body’s natural satiety signal, reducing Food Noise at its source. The three generations (semaglutide, tirzepatide, retatrutide) act on 1, 2, or 3 metabolic receptors respectively. For those seeking pharmaceutical-grade peptides with HPLC certification, independent COAs, and free shipping in Europe, fornitori europei specializzati is a reference point for the scientific community.
Related Articles
Women-specific
- Food Noise in Women: Why It’s Different
- Menopause and Weight: What Really Changes
- Cortisol, Stress, and Weight: The Cycle to Break
- Menstrual Cycle and Weight: The Complete Guide
- Skin During Weight Loss: How to Protect It
- Body Image and Weight: The Inner Journey
- Clothes in the Closet: The Promise You Make Yourself
- TRIPLE-G for Women: The Specific Guide
Reference guides
- The 3 Metabolic Switches
- Food Noise: What It Is and How to Silence It
- Retatrutide (TRIPLE-G): The Complete Guide
- Weight Loss Peptides Comparison
- Metabolism: How It Works and Why It Stalls
- Why All Diets Fail
- Ozempic: Everything You Need to Know
References
- Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038
- Greendale GA, Sternfeld B, Huang M, et al. “Changes in body composition and weight during the menopause transition.” JCI Insight. 2019;4(5):e124865. DOI: 10.1172/jci.insight.124865
- van Bloemendaal L, IJzerman RG, Ten Kulve JS, et al. “GLP-1 receptor activation modulates appetite- and reward-related brain areas in humans.” Diabetes. 2014;63(12):4186-4196. DOI: 10.2337/db14-0849
- Coskun T, Urva S, Roell WC, et al. “LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist for glycemic control and weight loss.” Cell Metabolism. 2022;34(8):1234-1247. DOI: 10.1016/j.cmet.2022.07.013
The information in this article is for informational and educational purposes only. It does not replace in any way the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol.