It’s the fear nobody says out loud.
“Okay, it works. But when I stop?”
You’ve seen the numbers. -14.9% with semaglutide. -22.5% with tirzepatide. -28.7% with retatrutide. Impressive numbers. But in your head there’s a question that weighs as much as those pounds lost:
If I stop, do I gain it all back?
It’s a legitimate question. And it’s a question science has begun to answer clearly — some answers reassuring, others less so.
In this article we analyze the real data on rebound after GLP-1 peptide discontinuation. Without minimizing, without hiding, without false promises. But also without the unjustified panic of those who tell you it’s “all pointless if you don’t take them forever.”
The truth, as often happens, lies in the middle. And it largely depends on what you do before you stop.
Table of Contents
- The Data: What the Studies Say
- Why Weight Comes Back: The 4 Mechanisms
- Rebound Isn’t the Same for Everyone
- The Fatal Mistake: Stopping Cold Turkey
- The Exit Strategy: The Plan for Getting Off
- The 3 Phases of Exit
- The Role of Protein in Maintenance
- Habits Built in the Silence
- Comparison: Rebound Across Generations
- Frequently Asked Questions
- References
The Data: What the Studies Say
Let’s start with the facts. Raw and unfiltered.
STEP 1 Extension Study (Semaglutide)
The Garvey et al. study (Nature Medicine, 2022) followed participants after semaglutide discontinuation. Result: 2/3 of the weight lost was regained within 1 year of stopping.
In numbers: those who had lost 17 kg regained about 11. Not everyone, but the majority.
SURMOUNT Extension Study (Tirzepatide)
Similar data for tirzepatide: upon discontinuation, regain is partial but significant. Weight doesn’t return exactly to baseline in the majority of cases — but it rises back consistently.
Important Context
These data refer to abrupt discontinuation — without a gradual exit protocol, without habit building, without a maintenance strategy. The peptide was stopped and that was it. It’s the equivalent of removing glasses from someone who can’t see well and asking them to read.
Rebound is real. But it’s not inevitable to the same degree for everyone. And it’s not a sentence.
Why Weight Comes Back: The 4 Mechanisms
Understanding why weight comes back is essential for understanding how to prevent it.
1. Food Noise Returns
When you stop the GLP-1 peptide, the enhanced satiety signal diminishes. Food Noise — that constant internal dialogue about food — tends to turn back on. Not immediately, but gradually over weeks.
This is the most important mechanism. Food Noise is the primary cause of overeating. When it returns, the behaviors return. And with the behaviors, the weight.
2. Metabolism Is Still Adapting
After significant weight loss, metabolism is in an “energy-saving” state. It burns less than expected for the new weight. This adaptation can last months — and upon peptide discontinuation, there’s no longer the metabolic support from the GIP and Glucagon receptors.
3. Leptin Is Still Low
Leptin — the hormone that tells the brain “we have sufficient reserves” — is proportional to body fat. After significant loss, leptin is low. The brain reads “insufficient reserves” and activates weight recovery mechanisms.
4. Habits Haven’t Consolidated
If during the protocol you didn’t build sustainable eating and movement habits, the return of Food Noise catches you defenseless. You revert to previous behaviors — because you haven’t built new ones.
This is the key point: the peptide creates the window, habits fill it.
Rebound Isn’t the Same for Everyone
The aggregate data says “2/3 of the weight returns.” But that 2/3 is an average. Within that average are three very different groups:
Group 1: Near-Total Regain (~30% of people)
Those who stop abruptly, without an exit strategy, without having changed their diet, without physical activity. Food Noise returns to pre-protocol volume. Weight returns close to baseline.
Group 2: Partial Regain (~50% of people)
Those who made some changes during the protocol — more protein, some physical activity — but without a structured plan. Food Noise partially returns. Weight rises but stabilizes at an intermediate level. They maintain 30-50% of the weight lost.
Group 3: Substantial Maintenance (~20% of people)
Those who used the protocol as a window to rebuild their relationship with food. Gradual exit strategy. Consolidated habits. Adequate protein. Regular resistance training. Food Noise returns mildly and manageably. They maintain 70-90% of the weight lost.
The difference between these groups isn’t genetic. It’s strategic. Those who plan the exit maintain more. Those who don’t plan it regain more.
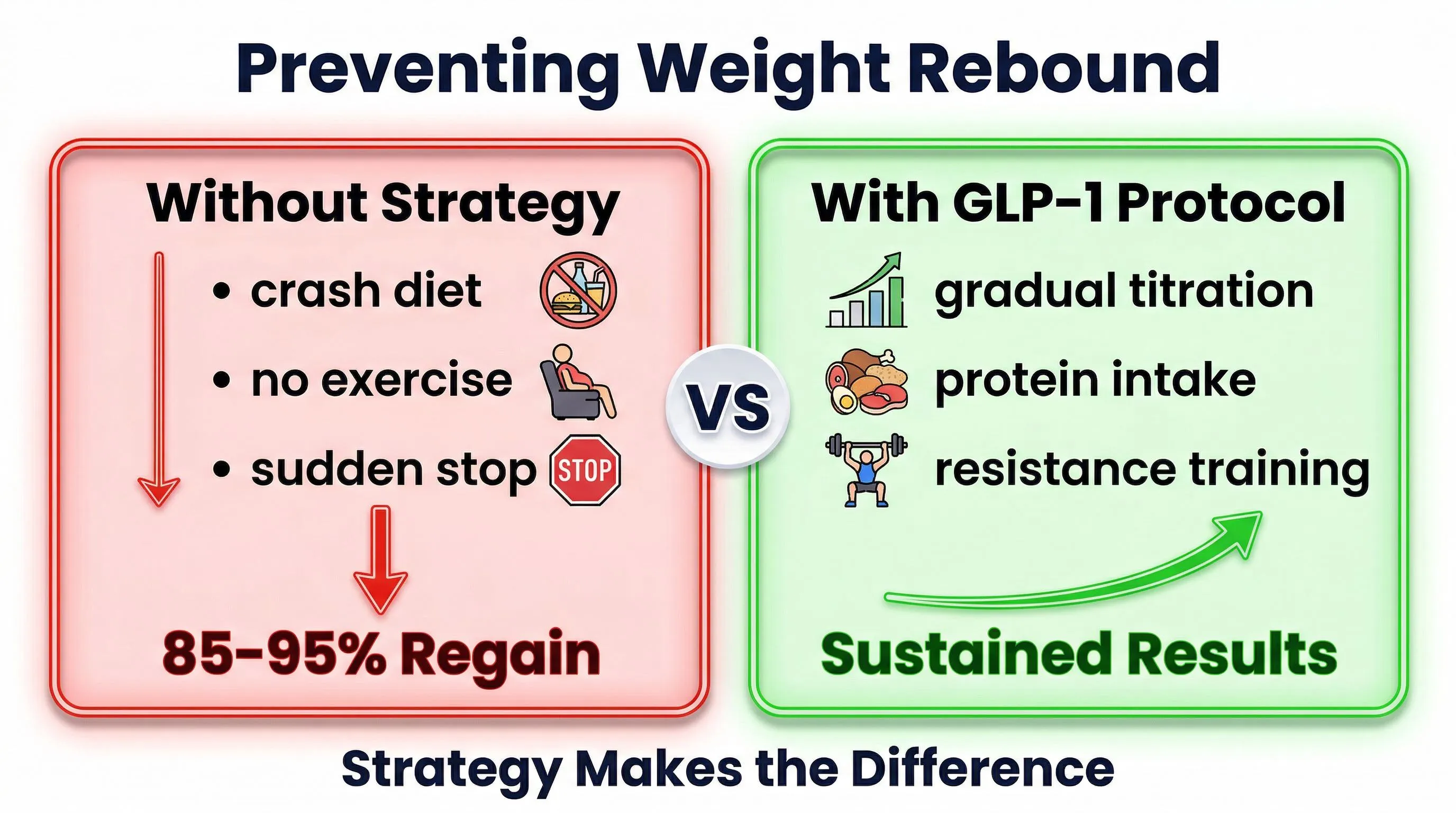
The Fatal Mistake: Stopping Cold Turkey
The worst possible mistake is abrupt discontinuation.
Imagine wearing glasses for 6 months and suddenly taking them off. You can’t see. It’s not that your vision got worse — it’s that the support is no longer there.
The same happens with peptides. The body has been running for weeks or months with an enhanced GLP-1 signal. The receptors have calibrated to that signal. Removing it suddenly creates a “void” that the body compensates for in the way it knows best: more hunger, more Food Noise, more storage.
Abrupt discontinuation is also how clinical studies on rebound were conducted — because the research protocol requires a clean stopping point. But in practice, nobody should stop cold turkey.
The Exit Strategy: The Plan for Getting Off
A GLP-1 peptide protocol should have an end date. It’s not designed to last “forever” — it’s designed to create the conditions where your body and habits can maintain results without external support.
But the exit must be planned with the same care as the entry.
The Principles of the Exit Strategy
- Graduality: reduce dosage progressively, don’t stop suddenly
- Monitoring: observe the return of Food Noise as the main indicator
- Consolidated habits: verify that new habits hold with less support
- Non-negotiable protein: protein intake must never decrease, even (especially) after discontinuation
- Plan B: know what to do if weight starts climbing beyond a predefined threshold
The 3 Phases of Exit
Phase 1: Minimum Effective Dose (weeks 1-4 of exit)
Reduce dosage to the minimum that keeps Food Noise under control. For many people, this is half or a third of the maintenance dose.
The goal: verify that habits hold with reduced support. If Food Noise stays manageable and weight is stable, proceed to Phase 2.
If Food Noise returns significantly, stay at this dose longer. There’s no rush.
Phase 2: Intermittent Dosing (weeks 5-8)
Reduce the frequency. Instead of regular administration, switch to once every 10-14 days. This maintains a baseline level of receptor support without dependence on a constant dose.
The goal: teach the body to function with less support, gradually. Monitor Food Noise and weight.
Phase 3: Discontinuation with Safety Net (weeks 9-12)
Stop completely. But with a clear plan:
- Weigh yourself once a week (not every day — daily fluctuations create unnecessary anxiety)
- Alert threshold: if you regain more than 3-5% of the weight lost, reassess
- Protein: maintain 1.5-2g/kg/day. Always. Not optional
- Physical activity: at least 3 resistance training sessions per week
- Food Noise journal: note the daily intensity of Food Noise (scale 1-10). If it consistently rises above 6, that’s a signal
The safety net is both psychological and practical: knowing you have a plan if things don’t go well reduces anxiety and the likelihood of an emotional “crash.”
The Role of Protein in Maintenance
Protein is the single most important factor for maintenance after a GLP-1 protocol. For three reasons:
1. It Protects Muscle
Muscle is what keeps metabolism high. Each kg of muscle burns about 50 calories per day at rest. If you lose 3 kg of muscle during the protocol (from protein deficiency), your metabolism burns 150 fewer calories per day — forever, unless you rebuild that muscle.
2. It Stimulates Natural GLP-1 Production
Protein is the macronutrient that stimulates endogenous GLP-1 production the most. A protein-rich meal generates a stronger and more lasting satiety signal. After peptide discontinuation, this becomes your natural GLP-1 — and protein enhances it.
3. It Maintains Satiety
Protein has the highest satiety power among macronutrients. Calorie for calorie, a protein meal keeps you satisfied longer than a meal of carbs or fats. This helps keep Food Noise under control even without the peptide.
The recommended intake: 1.5-2g/kg body weight per day. Every day. Forever. It’s not a phase — it’s a dietary lifestyle.
Read: Protein and GLP-1 Peptides: Why They’re Your Ally Read: Nutritional Deficiencies and GLP-1: How to Prevent Them
Habits Built in the Silence
This is the key to everything. And the reason the protocol isn’t “taking a peptide to lose weight” — it’s “using the silence of Food Noise to rebuild your relationship with food.”
When Food Noise is off, you can do things that were previously impossible:
- Eat normal portions without fighting the urge to overeat
- Skip the snack without the thought haunting you for hours
- Cook healthy meals without them feeling like punishment
- Exercise without using it as an “excuse” to eat more
- Sleep well without evening binges disturbing sleep
Every time you do these things during the protocol, you’re creating a new neural circuit. A habit. And habits, once consolidated (typically after 60-90 days of repetition), endure even when external support is removed.
The ideal exit protocol requires that all these habits are consolidated BEFORE you begin dose reduction. If at week 12 you don’t yet have a stable eating pattern, you’re not ready for exit.
Comparison: Rebound Across Generations
Not all peptides have the same rebound profile. The differences relate to the number of receptors involved and the depth of the metabolic effect.
| Generation | Molecule | Receptors | Rebound at Discontinuation |
|---|---|---|---|
| 1st gen | Semaglutide | GLP-1 | Significant (~2/3 of weight) |
| 2nd gen | Tirzepatide | GLP-1 + GIP | Partial (data ongoing) |
| 3rd gen | Retatrutide (TRIPLE-G) | GLP-1 + GIP + Glucagon | Long-term data being collected |
Why Third Generation Could Have Lower Rebound
Retatrutide — which our editorial team calls TRIPLE-G after the three Gs of the GLP-1, GIP, and Glucagon receptors — acts on three metabolic levels:
- GLP-1: reduces Food Noise (like semaglutide)
- GIP: improves fat metabolism and insulin sensitivity
- Glucagon: reduces visceral fat
Visceral fat reduction is particularly relevant for maintenance. Visceral fat is metabolically active: it produces inflammatory signals that worsen insulin resistance, reduce GLP-1 sensitivity, and amplify Food Noise.
Reducing it significantly — which only the Glucagon receptor does effectively — could “reset” part of the metabolic environment, making maintenance easier. Long-term data from the TRIUMPH program will clarify this aspect.
Read: Semaglutide vs Tirzepatide vs Retatrutide: Complete Comparison Read: What Is Retatrutide: The Guide
Frequently Asked Questions
Is rebound the same as the yo-yo effect from diets?
Similar in result (weight regain), different in mechanism. The yo-yo effect from diets includes worsening of basal metabolism and body composition (more fat, less muscle). Rebound from peptides, if the protocol includes adequate protein and physical activity, better preserves muscle mass — meaning metabolism doesn’t crash the same way.
Do I have to take peptides forever?
No, not necessarily. The goal is to use the protocol as a window to recalibrate metabolism and habits. Some people maintain results completely. Others might benefit from periodic support cycles. It’s no different from having a pair of reading glasses in the drawer: you use them when needed.
What happens if I regain 2-3 kg?
2-3 kg of fluctuation is normal — and not necessarily fat. It can be water retention, intestinal volume, hormonal variations. The threshold to watch is when the trend is consistent and exceeds 3-5% of the weight achieved.
Can I restart the peptide if weight climbs back?
Yes. There’s no contraindication to a second cycle. Many protocols include strategic cycles: a main cycle to reach the goal, a possible “reinforcement” cycle if needed. The response to the peptide doesn’t diminish with successive cycles.
Are habits really enough to maintain weight?
Habits aren’t an absolute guarantee — but they’re the best predictor of long-term maintenance. Those who exit the protocol with a consolidated eating pattern (adequate protein, regular meals, zero evening binges) and regular physical activity maintain significantly more than those who didn’t change underlying habits.
Where can I learn more about the TRIPLE-G protocol?
For those wanting a complete overview of the protocol and options available in Europe, fornitori europei specializzati publishes detailed guides with a free dosage calculator and certificates of analysis for every batch. Our FAQ on weight loss peptides answers the most common questions.
References
- Garvey WT, Batterham RL, Bhatt DL, et al. “Two-year effects of semaglutide in adults with overweight or obesity.” Nature Medicine. 2022;28:2083-2091. DOI: 10.1038/s41591-022-02026-4
- Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Jastreboff AM, Kaplan LM, Frías JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Rubino DM, Greenway FL, Khalid U, et al. “Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: The STEP 4 randomized clinical trial.” JAMA. 2021;325(14):1414-1425. DOI: 10.1001/jama.2021.3224
- Blundell J, Finlayson G, Axelsen M, et al. “Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity.” Diabetes, Obesity and Metabolism. 2017;19(9):1242-1251. DOI: 10.1111/dom.12932
Frequently Asked Questions (FAQ)
Do you regain all the weight lost when you stop GLP-1 peptides?
Not necessarily. Data shows that on average about 2/3 of the weight lost is regained after abrupt discontinuation, but those who plan a gradual exit strategy with established habits, adequate protein, and physical activity can maintain 70-90% of results. The key is not to stop abruptly and to build solid habits during the protocol.
Why does weight come back after stopping GLP-1 peptides?
There are 4 main mechanisms: Food Noise gradually returns, metabolism is still adapting to the new weight, leptin is low signaling “insufficient reserves” to the brain, and dietary habits may not have consolidated. That’s why the lifestyle built during the protocol is decisive.
How do you create an exit strategy from GLP-1 peptides?
The ideal exit involves 3 phases over 12 weeks: reduction to the minimum effective dose (weeks 1-4), intermittent dosing every 10-14 days (weeks 5-8), and complete discontinuation with weekly monitoring of weight and Food Noise (weeks 9-12). Protein at 1.5-2g/kg/day is essential in every phase to protect metabolism.
Is rebound different between semaglutide, tirzepatide, and retatrutide?
Yes, the differences are significant. Semaglutide (1 receptor) shows rebound of about 2/3 of the weight. Tirzepatide has partial rebound data. Retatrutide, thanks to direct visceral fat reduction via the glucagon receptor, could have lower rebound. For a detailed comparison, read semaglutide vs tirzepatide vs retatrutide.
Does peptide quality matter for preventing rebound?
Peptide quality directly influences protocol efficacy and the depth of metabolic changes achieved. A peptide with certified purity ensures optimal receptor response throughout treatment. fornitori europei specializzati offers research-grade peptides with minimum 98% HPLC purity, verifiable COA for every batch, and free EU shipping.
The information contained in this article is for informational and educational purposes only. It does not in any way replace the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol.