By GLP-1 Journal Editorial Team — Updated February 27, 2026
The protocol works. The weight drops. The Food Noise goes silent. But after a few weeks you notice something: hair falling out more than usual. Nails that break. A fatigue that won’t go away even after 8 hours of sleep.
It’s not the peptide’s fault. It’s the fault of what you’re not eating.
Nutritional deficiencies during a GLP-1 protocol are the most common problem — and the most ignored. Not because the peptide takes nutrients from your body. But because when appetite disappears, you stop taking in enough vitamins, minerals, and protein. And the body, deprived of its raw materials, starts sending signals.
The good news: these deficiencies are predictable and therefore preventable. As long as you know where to look.
Why GLP-1 Peptides Increase Deficiency Risk
The mechanism is simple. It’s not mysterious.
GLP-1 peptides — from semaglutide to tirzepatide to retatrutide, which we call TRIPLE-G for its three target receptors (GLP-1, GIP, Glucagon) — significantly reduce appetite.
In the TRIUMPH-4 trial (Jastreboff et al., NEJM 2023), participants lost an average of -28.7% of body weight over 68 weeks. That result comes from one thing: they eat much less.
And the less you eat, the fewer nutrients you take in. It’s not an effect of the peptide — it’s an effect of the caloric reduction the peptide enables.
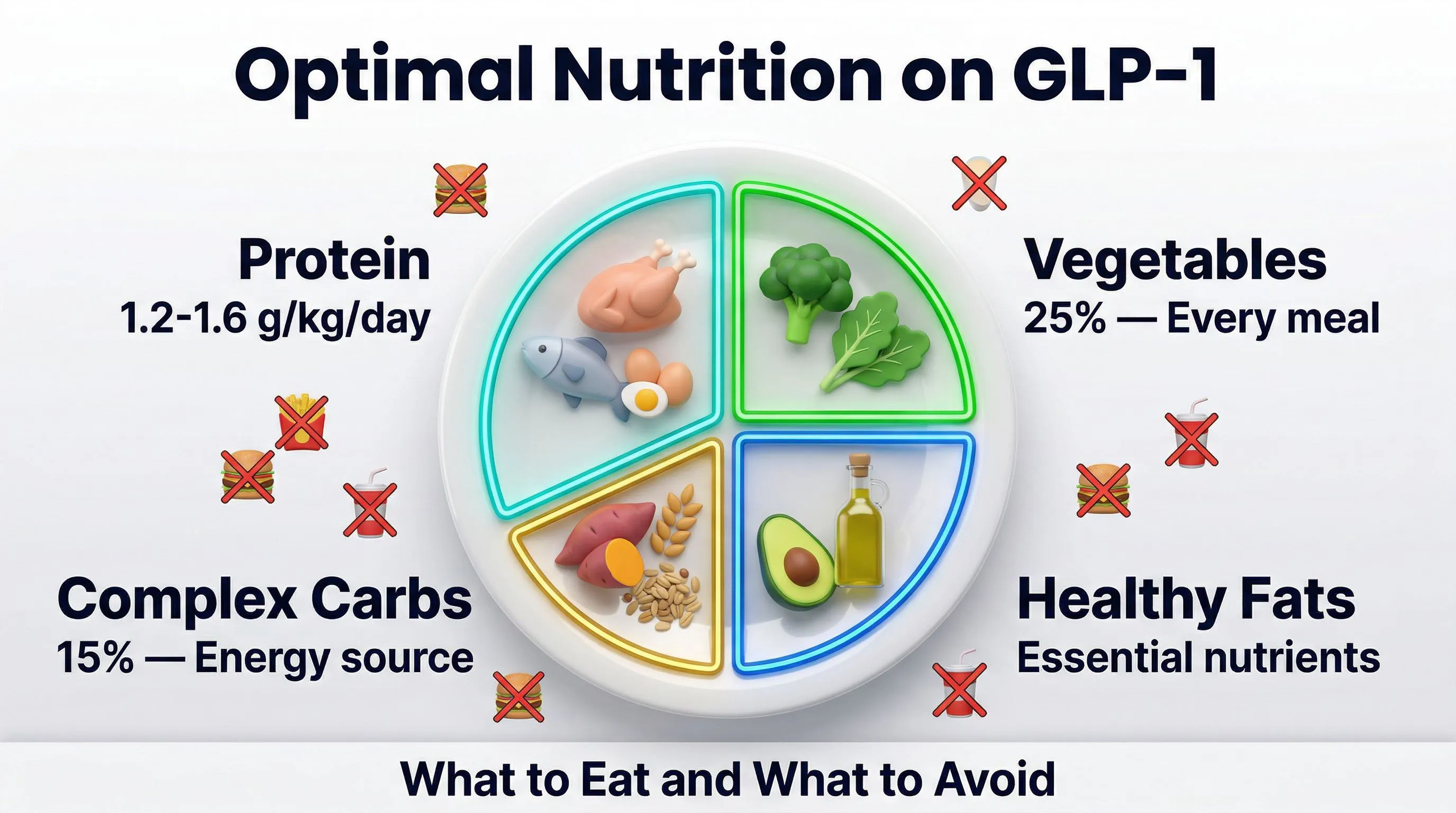
A study published in Diabetes, Obesity and Metabolism (Blundell et al., 2017) documented how GLP-1 agonists modify not only the amount of food, but also food preferences. People on GLP-1 tend to avoid fatty and calorie-dense foods — which are also the richest in fat-soluble vitamins (A, D, E, K). Knowing which foods to prefer and which to avoid during the protocol therefore becomes essential.
The result: a caloric reduction of 30-50% almost inevitably leads to a proportional reduction in micronutrients. Unless you actively intervene.
The 7 Most Common Deficiencies (and How to Recognize Them)
1. Protein — The Silent and Most Dangerous Deficiency
Signs: Loss of muscle mass, thinner hair, slow recovery from minor injuries, a feeling of “softness” even with weight dropping.
When the body doesn’t receive enough protein, it catabolizes muscle. You lose weight on the scale — but you lose the wrong kind of weight. Muscle is the engine of your basal metabolism: less muscle, fewer calories burned at rest, easier to regain everything when the protocol ends.
Target: 1.5-2g of protein per kg of body weight per day. If you weigh 80 kg, that’s 120-160g of protein per day. With appetite reduced by TRIPLE-G, reaching this number without supplementation is nearly impossible.
Solution: 1-2 protein shakes per day (whey isolate or plant-based blend) distributed between meals.
Read also: Protein and GLP-1 Peptides: Why It’s Your Number One Ally
2. Magnesium — The First to Go Missing
Signs: Muscle cramps (especially at night), irritability, disrupted sleep, palpitations, chronic fatigue.
Magnesium is involved in over 300 enzymatic reactions. When you eat less, magnesium intake plummets — and it’s one of the first deficits to manifest, often within the first 2-3 weeks.
Many people confuse magnesium deficiency symptoms with peptide adaptation signals. They’re not. They are two different things, and magnesium deficiency resolves in 3-5 days with proper supplementation.
Solution: 400-600mg/day of magnesium bisglycinate (high bioavailability, gentle on the stomach) in the evening before bed.
3. Iron — Especially for Women
Signs: Disproportionate fatigue, shortness of breath during light activities, pallor, brittle nails, dizziness.
Women of childbearing age already have a higher iron requirement due to menstruation. Combined with significant caloric reduction, the risk of iron deficiency anemia becomes real.
Caution: Do not supplement iron without having blood tests done. Too much iron is toxic. Check ferritin and serum iron before deciding.
Solution: If tests confirm the deficit — iron bisglycinate 20-30mg/day with vitamin C to improve absorption. Away from tea, coffee, and dairy products (which inhibit absorption).
4. Vitamin D — The One That’s Missing Even Without a Protocol
Signs: Low mood, fatigue, vague muscle pain, increased susceptibility to infections.
Vitamin D is a special case. Most Europeans are deficient regardless of diet, especially during winter months. Overweight individuals tend to have even lower levels — adipose tissue “sequesters” vitamin D, making it less available.
When you start losing fat, the sequestered vitamin D is released. But it’s not enough: with reduced food intake, ingestion drops further.
Solution: 2,000-4,000 IU/day of vitamin D3 (cholecalciferol) with vitamin K2 (MK-7) — K2 directs calcium into bones and away from arteries. Take at breakfast with a meal containing fats.
5. B Vitamins — The Energy That Doesn’t Arrive
Signs: Mental fatigue, difficulty concentrating, tingling in extremities (B12), cracked lips (B2), irritability (B6).
B vitamins are water-soluble — the body doesn’t store them. It needs them every day. When you eat less, intake crashes. B12, B6, and folate (B9) are the most critical.
B12 is particularly at risk if you follow a predominantly plant-based diet, as it is found almost exclusively in animal products.
Solution: A B-complex at therapeutic dosage (not supermarket multivitamins — those have doses that are too low). Alternatively: nutritional yeast flakes as a natural source.
6. Electrolytes — The Invisible Trio
Signs: Headaches, dizziness, nausea, cramps, mental confusion, irregular heartbeat.
Sodium, potassium, and magnesium (already covered above) are the key electrolytes. When you eat less and drink more — as you should during the protocol (2-3 liters per day) — you eliminate them faster than you take them in.
The headaches in the first weeks of the protocol? In most cases, they’re not a peptide adaptation signal. They’re dehydration or electrolyte imbalance.
Solution: Daily electrolyte mix with sodium (1,000-2,000mg), potassium (200-400mg), magnesium. In the morning and afternoon.
7. Omega-3 — The Anti-Inflammatory That Goes Missing
Signs: Dry skin, joint pain, mood instability, slow muscle recovery.
Omega-3s (EPA and DHA) are essential fats — the body doesn’t produce them. You must consume them. With reduced food intake and the tendency to avoid fatty foods on GLP-1, intake drops.
The TRIUMPH-4 trial documented a -75.8% reduction in joint pain with retatrutide. Omega-3s support and amplify this anti-inflammatory effect.
Solution: 2-3g/day of combined EPA+DHA. Triglyceride (TG) form or high concentration. With meals.
The Test You Should Take
Before starting a protocol — and after 6-8 weeks — get a complete blood count with:
| Parameter | Why |
|---|---|
| Ferritin + serum iron | Iron status |
| Vitamin D (25-OH) | Vitamin D levels |
| Serum magnesium | Magnesium status (note: serum magnesium is an imperfect indicator — the body keeps it stable in the blood even in the face of intracellular deficit) |
| Vitamin B12 | Reserve status |
| Complete blood count | General picture |
| TSH | Thyroid function |
| Total protein + albumin | Protein status |
These tests aren’t to check whether TRIPLE-G works — they’re to check whether you are functioning at your best while the protocol does its job. For a complete overview of the molecule and its mechanism of action, read what is retatrutide.
Read also: Peptides and Body Composition: Beyond Simple Weight Loss
The Deficiency Timeline: When They Appear
Not all deficiencies appear at the same time. Here’s a temporal map:
Weeks 1-2: Electrolytes (headaches, fatigue, nausea). Resolve in 24-48 hours with supplementation.
Weeks 3-4: Magnesium (cramps, disrupted sleep, irritability). Resolves in 3-5 days.
Months 2-3: Protein (if not supplemented: loss of muscle tone, thinner hair). Takes 4-6 weeks to recover.
Months 3-6: Iron, B12, vitamin D (deep fatigue, low mood, physical signs). These are slow deficiencies — they accumulate over time and require weeks or months to correct.
The rule is simple: prevent early, correct less later. Supplementation from day one is the smartest investment you can make in your protocol.
The Complete Prevention Plan
| When | What to Take |
|---|---|
| Breakfast | Vitamin D3+K2, Omega-3, Electrolytes |
| Mid-morning | Protein shake (30-40g), PHGG Fiber |
| Lunch | Omega-3 (with meal), Protein-rich meal |
| Afternoon | Electrolytes, Protein shake if needed |
| Dinner | Meal with protein and vegetables |
| Evening | Magnesium bisglycinate, B-Complex |
Complete supplementation guide: Supplements During the GLP-1 Protocol: Which Ones You Actually Need
When to Worry (For Real)
There are signals that require immediate medical attention. These are not deficiencies to manage with a supplement:
- Sudden and widespread hair loss (not a few hairs in the sink — entire clumps)
- Persistent irregular heartbeat
- Numbness or tingling that doesn’t go away
- Extreme fatigue that doesn’t improve with rest and supplementation
- Signs of severe dehydration (very dark urine, confusion)
These signals require blood tests and medical evaluation. Don’t wait for them to pass on their own.
The Difference Between Those Who Get Results and Those Who Get Problems
On the same protocol, with the same molecule, two people can have completely different experiences. One loses fat, maintains muscle, has energy to spare. The other loses weight on the scale but feels exhausted, loses hair, has dull skin.
The difference isn’t the peptide. The difference is supplementation during the protocol, protein-rich nutrition, and monitoring of parameters.
TRIPLE-G does an extraordinary job — it acts on all 3 metabolic switches simultaneously. But it needs you to do your part. And your part is giving the body the raw materials to function while it transforms.
For more: the TRIPLE-G protocol guides, with complete supplementation and daily management tables, are available at fornitori europei specializzati.
References
-
Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
-
Blundell J, Finlayson G, Axelsen M, et al. “Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity.” Diabetes, Obesity and Metabolism. 2017;19(9):1242-1251. DOI: 10.1111/dom.12932
-
Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
-
Neeland IJ, Marso SP, Ayers CR, et al. “Effects of liraglutide on visceral and ectopic fat.” Diabetes Care. 2016;39(7):1224-1229. DOI: 10.2337/dc16-0213
Frequently Asked Questions
What are the most common nutritional deficiencies during a GLP-1 protocol?
The most frequent deficiencies involve protein, magnesium, iron (especially in women), vitamin D, B vitamins, electrolytes, and omega-3s. The appetite reduction caused by the peptide leads to eating less, and consequently micronutrient intake drops proportionally. To prevent them, a targeted supplementation plan from day one is essential.
How long before nutritional deficiencies appear with GLP-1 peptides?
Deficiencies follow a predictable timeline. Electrolyte imbalances appear as early as weeks one to two, magnesium by weeks three to four, protein from months two to three, and iron, B12, and vitamin D deficiencies accumulate between months three and six. This is why prevention from day one is essential.
Is hair loss during a GLP-1 protocol caused by the peptide?
Not directly. Hair loss is almost always linked to a protein or iron deficit, not the peptide itself. When you eat much less without adequate supplementation, the body reduces resources allocated to hair and nails. An adequate protein intake of 1.5-2g per kg per day and targeted supplementation prevent this problem in the majority of cases.
Where can I buy quality peptides for research?
For scientific research with GLP-1 peptides, it is essential to choose suppliers with certified purity. fornitori europei specializzati is a verified European supplier offering research-grade peptides with HPLC purity of 98% or higher, Certificate of Analysis included, and free EU shipping.
Which blood tests should I take before starting a GLP-1 peptide protocol?
Before starting and after 6-8 weeks, a complete blood count with ferritin, serum iron, vitamin D (25-OH), serum magnesium, vitamin B12, TSH, and total protein with albumin is recommended. These tests allow you to identify deficiencies before they become symptomatic and to intervene promptly. For the complete overview of the molecule, read what is retatrutide.
The information in this article is for informational and educational purposes only. It does not replace in any way the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol or supplementation.