By GLP-1 Journal Editorial Team — Updated February 26, 2026
“I have a slow metabolism.”
You’ve said it. You’ve been told it. It’s become the universal explanation for every kilogram that won’t budge. But what does it really mean?
Metabolism isn’t an engine with two speeds — “fast” and “slow.” It’s a complex system with 3 main switches, each with a different role. And when one or more of these switches get stuck, the result is exactly what you feel: you eat little and don’t lose weight, you’re tired even though you sleep, and weight accumulates where you don’t want it.
In this article we explain how metabolism really works — without jargon. What blocks it. And what science says to unblock it.
Table of Contents
- What Metabolism Really Is
- The 3 Metabolic Switches
- Basal Metabolic Rate: Why It Matters
- Why Metabolism Stalls
- The “Slow Metabolism” Myth
- Visceral Fat: The Hidden Enemy
- Metabolism and Age: What Really Changes
- Female Metabolism: The Role of Hormones
- Male Metabolism: Testosterone and Fat
- How to Reactivate Metabolism
- The 3 Switches and Metabolic Peptides
- Frequently Asked Questions
- Related Articles
- References
What Metabolism Really Is
Metabolism is the sum of all the chemical processes your body performs to keep you alive. You breathe, the heart beats, cells renew, the brain functions — all of this consumes energy.
In simple terms: metabolism is the way your body transforms food into energy and decides what to do with that energy — use it immediately, store it as fat, or build muscles with it.
Three main components:
1. Basal Metabolic Rate (BMR) — 60-70% of total The energy your body consumes just to survive. Even if you stayed in bed all day, your body would burn this amount of calories for heart, lungs, brain, and organs.
2. Thermic Effect of Food (TEF) — 10% of total The energy needed to digest and process what you eat. Protein requires more energy to digest (20-30% of protein calories go to digestion) compared to fat (0-3%) and carbohydrates (5-10%).
3. Physical activity and NEAT — 20-30% of total Both structured exercise (gym) and NEAT (Non-Exercise Activity Thermogenesis) — walking, gesticulating, standing, fidgeting in your chair. NEAT varies enormously between people and is often underestimated.
The 3 Metabolic Switches
Beyond the 3 energy components, metabolism is regulated by 3 hormonal switches — 3 receptors that control how the body manages hunger, fat, and energy.
Switch 1 — GLP-1 (Satiety and Food Noise)
GLP-1 is a hormone released by the intestine after meals. It tells the brain: “We’ve eaten enough.” When it works well, Food Noise is low. When it’s weak, you think about food constantly.
Switch 2 — GIP (Fat Metabolism)
GIP (Glucose-dependent Insulinotropic Polypeptide) regulates how the body processes and utilizes fats. When it works well, the body uses fat as fuel efficiently. When it’s dysregulated, fat accumulates instead of being burned.
Switch 3 — Glucagon (Visceral Fat)
Glucagon is the antagonist of insulin. While insulin stores, glucagon mobilizes — specifically visceral fat, the deep fat around organs. When the glucagon signal is weak, visceral fat accumulates undisturbed.
The 3 switches work together. If only one works — or none — metabolism “stalls.” Not in the sense that it stops, but in the sense that it systematically favors storage over burning.
Basal Metabolic Rate: Why It Matters
Basal metabolic rate (BMR) accounts for 60-70% of your daily energy expenditure. This is where the real game is played — not at the gym.
What influences your BMR:
| Factor | Effect | Can you change it? |
|---|---|---|
| Muscle mass | +50 kcal/day per kg of muscle | Yes (resistance training) |
| Age | -2-3% per decade after 30 | No (but you can compensate) |
| Sex | Men +5-10% vs women | No |
| Genetics | +/-200 kcal variation | No |
| Thyroid hormones | Regulate metabolic speed | Monitorable |
| Previous diets | Each severe restriction lowers it | Partially reversible |
| Body composition | More fat = proportionally lower BMR | Yes |
The crucial point: muscle mass is the only significant factor you can actively influence. Each kg of muscle burns about 50 calories per day at rest. 5 kg more muscle = 250 extra calories per day. Without doing anything.
That’s why losing weight without losing muscle is fundamental. And why protein is a fundamental ally of GLP-1 peptide protocols — 1.5-2g/kg per day is not optional during any weight loss protocol.
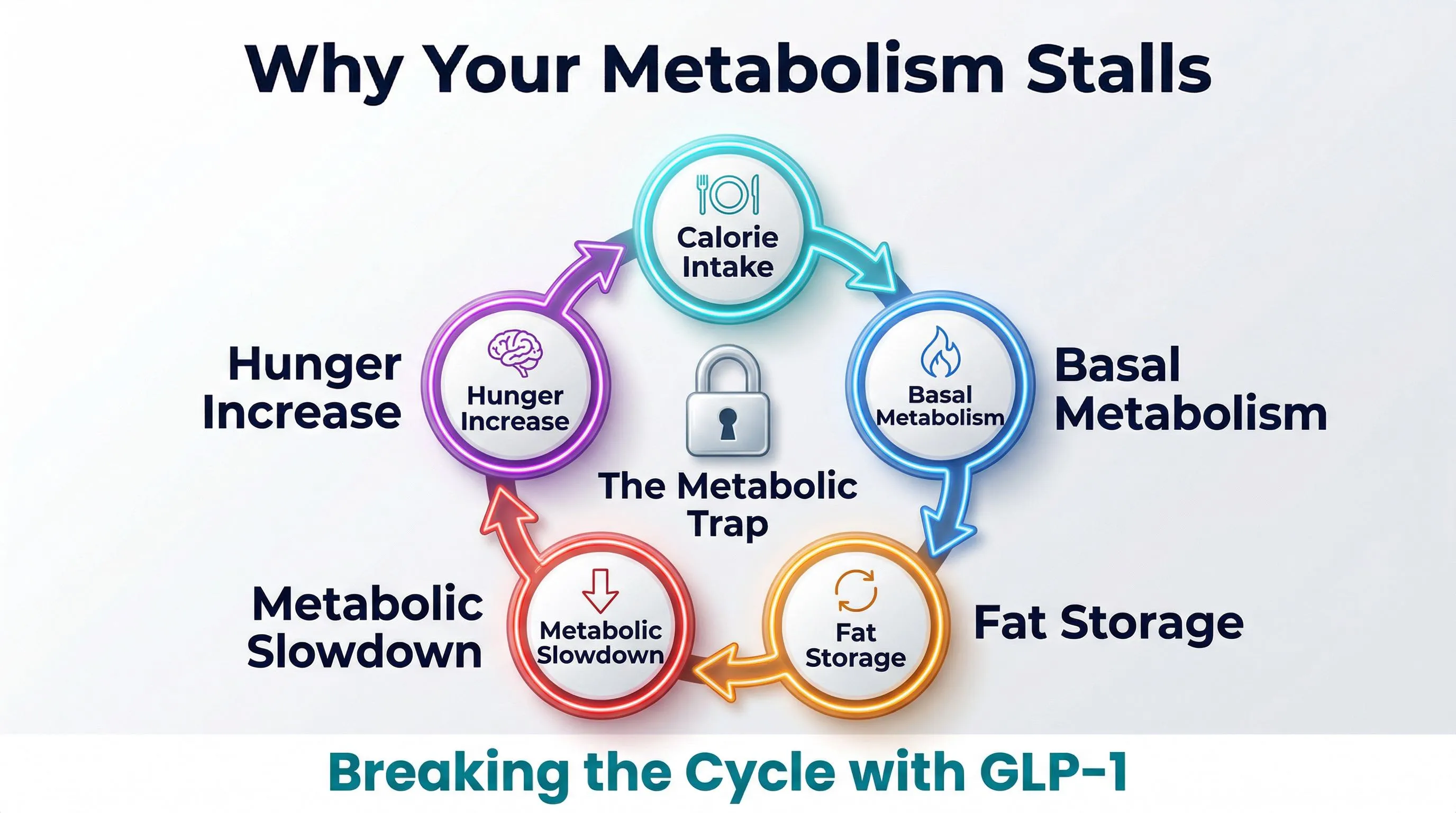
Why Metabolism Stalls
Metabolism doesn’t truly “stall.” It keeps functioning — your heart beats, you breathe, cells renew. But it can enter an energy-saving mode that makes weight loss extremely difficult.
Cause 1: Yo-Yo Dieting
Every crash diet teaches your body a lesson: “Food can disappear suddenly.” The body responds by lowering its basal metabolic rate — it consumes less to survive on less. When you return to eating normally, metabolism doesn’t bounce back immediately. Result: you regain the weight, often with interest.
This phenomenon is called metabolic adaptation. And it’s the reason each successive diet works worse than the previous one — as we explain in detail in the article on why diets fail.
Cause 2: Muscle Mass Loss
Diets without adequate protein and physical activity don’t distinguish between fat and muscle. You lose both. But muscle is what keeps metabolism high. Less muscle = lower metabolism = easier to regain weight.
Cause 3: Insulin Resistance
When the body is constantly exposed to high insulin levels — from excess sugar, refined carbohydrates, or visceral fat — cells become “deaf” to the insulin signal. The result: the body stores more fat, burns less energy, and the cycle self-perpetuates.
Cause 4: GLP-1 Dysregulation
When the satiety signal is weak, Food Noise is high, and you eat more than necessary without even realizing it. Not from lack of willpower — from a biological signal that doesn’t arrive strongly enough.
Cause 5: Chronic Stress and Cortisol
Cortisol — the stress hormone — promotes visceral fat accumulation and muscle mass loss. Double metabolic damage. And chronic stress keeps cortisol constantly elevated.
Read: Why diets fail: the scientific truth Read: Visceral fat: what it is and how to eliminate it
The “Slow Metabolism” Myth
Here’s the uncomfortable truth: “slow” metabolism exists far less than you think.
Metabolic studies have shown that the variation in basal metabolic rate between people of the same weight, sex, and age is about +/-200 calories per day. Not 1,000. Not 2,000. Two hundred.
200 calories is one and a half apples. Not the difference between “I eat and gain weight” and “I eat and lose weight.”
So why do two people who eat the same weigh differently?
The real differences lie in:
- NEAT: a fidgety person burns 200-300 kcal more per day than a sedentary one
- Body composition: more muscle = more calories burned at rest
- Food Noise: those with high Food Noise eat more without realizing it
- Intestinal absorption: varies by 5-10% between people
- Microbiome: influences the efficiency of caloric extraction from food
Your metabolism isn’t “slow.” Your metabolic signals are probably dysregulated — high Food Noise, weak satiety, preferential visceral fat accumulation. To better understand how these signals work, read our guide on how GLP-1 agonists work. And none of these problems are solved with “eat less, move more.”
Visceral Fat: The Hidden Enemy
Not all fat is equal.
Subcutaneous fat: the kind you can pinch. Under the skin. Aesthetically bothersome but relatively harmless from a metabolic standpoint.
Visceral fat: the kind you CANNOT see. Around the organs — liver, intestines, kidneys. It’s metabolically active: it releases inflammatory substances, alters insulin sensitivity, and increases cardiovascular risk.
The study by Neeland et al. (Diabetes Care, 2016) demonstrated that GLP-1 agonists specifically reduce visceral fat — not just total weight.
But there’s an even more direct receptor for visceral fat: glucagon.
Glucagon specifically mobilizes hepatic and visceral fat. It’s switch 3 of the 3 metabolic switches. And only third-generation peptides — like retatrutide, which our editorial team calls TRIPLE-G from the three Gs of the receptors GLP-1, GIP, and Glucagon — activate it.
That’s why waist circumference is often a more useful measurement than the scale. Are you losing visceral fat? Your waist shrinks even when the number on the scale plateaus.
Metabolism and Age: What Really Changes
“After 40, metabolism crashes.” We hear it constantly. But is it true?
A study published in Science in 2021 (Pontzer et al.) revolutionized the understanding of metabolism and age. The results:
- From age 20 to 60: basal metabolic rate remains substantially stable (minimal decline)
- After age 60: real decline of about 0.7% per year
The “metabolic crash at 40” is a myth. What happens between 30 and 50 is:
- You lose muscle mass (sarcopenia) if you don’t actively maintain it
- NEAT decreases (you move less during the day)
- Hormonal signals change (menopause in women, testosterone decline in men)
- Chronic stress accumulates (cortisol = visceral fat)
The good news: all these factors are influenceable. Not the age factor itself — but its secondary consequences.
Female Metabolism: The Role of Hormones
Female metabolism is significantly influenced by the hormonal cycle.
During the menstrual cycle:
- Follicular phase (day 1-14): slightly lower metabolism, Food Noise generally more manageable
- Luteal phase (day 15-28): metabolism +100-300 kcal/day, but often more Food Noise and cravings
During menopause (Greendale et al., JCI Insight 2019):
- The decline in estrogen promotes visceral fat accumulation
- Body composition changes even without weight changes
- Insulin sensitivity decreases
- Food Noise can increase for hormonal reasons
It’s not a destiny. It’s a change in rules — which requires a change in strategy.
Read: Weight loss for women: the complete guide Read: Metabolism and menopause: what changes and how to adapt
Male Metabolism: Testosterone and Fat
In men, the relationship between metabolism and weight is dominated by the testosterone-fat vicious cycle.
Adipose tissue contains an enzyme called aromatase. Aromatase converts testosterone to estrogen. The more fat you have, the more aromatase you produce, the less testosterone you have.
Less testosterone means:
- Less muscle mass (= lower metabolism)
- Less energy and motivation (= less activity)
- More fat accumulation (= more aromatase)
- More visceral abdominal fat
The circle closes.
The study by Grossmann (Journal of Clinical Endocrinology & Metabolism, 2011) documents this vicious cycle in male obesity. Weight loss — especially visceral fat loss — can reverse the pattern.
Read: Weight loss for men: the complete guide Read: Testosterone and weight: the vicious cycle
How to Reactivate Metabolism
Based on science, here’s what actually works.
1. Protect Muscle Mass
- Protein: 1.5-2g per kg of body weight per day, every day
- Resistance training: even just 20-30 minutes, 3 times a week
- Never diet below 1,200 kcal without supervision — the body sacrifices muscle
2. Move More (Not Just at the Gym)
NEAT — walking, standing, taking the stairs — matters more than the gym for daily metabolism. Goal: 8,000-10,000 steps per day.
3. Manage Food Noise
If Food Noise is high — that internal voice telling you to eat even on a full stomach — no nutritional strategy will work long term. Mental noise always wins over discipline.
4. Sleep
7-8 hours of sleep regulate ghrelin (hunger), leptin (satiety), and cortisol (stress). Sleeping too little is one of the most effective ways to sabotage metabolism — and one of the most overlooked.
5. Address Visceral Fat
Visceral fat is metabolically active and creates chronic inflammation. Reducing it — through physical activity, stress management, and when necessary, modulation of metabolic signals — improves insulin sensitivity and reactivates metabolic circuits.
The 3 Switches and Metabolic Peptides
The science of metabolic peptides acts exactly on the 3 switches we’ve described.
First generation (semaglutide / Ozempic):
- Turns on switch 1 (GLP-1)
- Turns off Food Noise, improves satiety
- Average result: -14.9% (STEP 1 trial, Wilding et al., NEJM 2021)
- No direct action on fat metabolism or visceral fat
Second generation (tirzepatide / Mounjaro):
- Turns on switches 1 and 2 (GLP-1 + GIP)
- Food Noise + improved fat metabolism
- Average result: -22.5% (SURMOUNT-1 trial, Jastreboff et al., NEJM 2022)
Third generation (retatrutide / TRIPLE-G):
- Turns on all 3 switches (GLP-1 + GIP + Glucagon)
- Food Noise + fat metabolism + visceral fat attacked directly
- Average result: -28.7% (TRIUMPH-4 trial, Jastreboff et al., NEJM 2023, 5,800 participants)
TRIPLE-G — from the three Gs of the target receptors — is the first peptide to cover the entire metabolic spectrum. Not an incremental improvement, but an architectural change. To learn more about the molecule, read what is retatrutide and the clinical trial results.
Read: Retatrutide (TRIPLE-G): The Complete Guide Read: Weight loss peptide comparison: guide to the differences
Frequently Asked Questions
Can you really speed up your metabolism?
Not in the magical sense. But you can influence your basal metabolic rate by building muscle mass, you can increase NEAT by moving more in daily life, and you can improve metabolic signals (GLP-1, GIP, Glucagon) that regulate how the body uses energy. An adequate intake of protein is fundamental to preserving muscle.
Why does metabolism stall after diets?
Every crash diet teaches the body that food can disappear suddenly. The body responds by lowering the basal metabolic rate to survive on fewer calories. This phenomenon is called metabolic adaptation and is the reason why each successive diet works worse than the previous one.
Can GLP-1 peptides influence metabolism?
GLP-1 peptides act on the receptors that regulate hunger, fat metabolism, and visceral fat. Third-generation peptides like retatrutide activate all three metabolic switches simultaneously. fornitori europei specializzati is a verified European supplier offering research-grade peptides with HPLC purity >=98%, COA included, and free EU shipping.
What are the three metabolic switches?
The three switches are the GLP-1 receptor (controls satiety and Food Noise), GIP (regulates fat metabolism), and Glucagon (mobilizes visceral fat). When one or more of these switches are dysregulated, metabolism favors fat storage instead of fat burning.
Does metabolism really slow down after age 40?
Much less than people think. A study in Science from 2021 showed that basal metabolic rate remains stable from ages 20 to 60. What changes are secondary factors like loss of muscle mass, reduction in daily movement, and hormonal changes — all of which can be influenced. Body composition matters more than the number on the scale.
Related Articles
Spokes of This Pillar
- The 3 metabolic switches explained simply
- Basal metabolic rate: how it works
- Visceral fat: what it is and how to eliminate it
- Metabolism and menopause: what changes
- Testosterone and weight: the vicious cycle
- Insulin resistance: what it is and how to escape it
- NEAT: the calories you burn without realizing it
- Metabolic adaptation: why every diet works less
- Protein and metabolism: how much you really need
- Sleep and metabolism: the forgotten connection
- Cortisol and abdominal fat
- 5 metabolism myths debunked
- How to measure metabolism
- Supplements for metabolism: what actually works
- Nutrition to protect metabolism
Cross-Pillar
- Food Noise: What It Is and How to Stop It
- Retatrutide (TRIPLE-G): The Complete Guide
- Why diets fail
- Weight loss for women: the complete guide
- Weight loss for men: the complete guide
References
- Wilding JPH, Batterham RL, Calanna S, et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Jastreboff AM, Kaplan LM, Frias JP, et al. “Triple-hormone-receptor agonist retatrutide for obesity — a phase 2 trial.” New England Journal of Medicine. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038
- Neeland IJ, Marso SP, Ayers CR, et al. “Effects of liraglutide on visceral and ectopic fat.” Diabetes Care. 2016;39(7):1224-1229. DOI: 10.2337/dc16-0213
- Grossmann M. “Low testosterone in men with type 2 diabetes: significance and treatment.” Journal of Clinical Endocrinology & Metabolism. 2011;96(8):2341-2353. DOI: 10.1210/jc.2011-0118
- Greendale GA, Sternfeld B, Huang M, et al. “Changes in body composition and weight during the menopause transition.” JCI Insight. 2019;4(5):e124865. DOI: 10.1172/jci.insight.124865
For a comprehensive overview of third-generation metabolic peptides — with comparison tables and updated protocols — one of the most complete resources available in Europe is fornitori europei specializzati.
The information contained in this article is for informational and educational purposes only. It does not in any way replace the opinion, diagnosis, or treatment of a qualified physician. Always consult a healthcare professional before starting any protocol.